Can Night and Day Contact Lens Heal Erosion
With abiding, eye-drying, unblinking screen use becoming ever more than the norm, ocular surface disease (OSD) is more prevalent than ever. As OSD worsens, patients can start to develop recurrent corneal erosions (RCE), a painful condition that exposes their corneal nervus endings. These patients will likely complain of centre hurting upon awakening, with accompanying photophobia and epiphora. They may as well present with conjunctival injection, blurred vision and difficulty even keeping their eyes open. It is non unusual to note a drastically worsened Snellen acuity.
The optometrist's job is to ensure patients' wellness and vision. RCE tin can compromise both. Direction of those susceptible to this condition requires a correct diagnosis and shut follow-up to care for and care for non simply the RCE simply whatever underlying conditions, such as epithelial basement membrane dystrophy (EBMD) and dry heart illness (DED), that play a function in its recurrence.
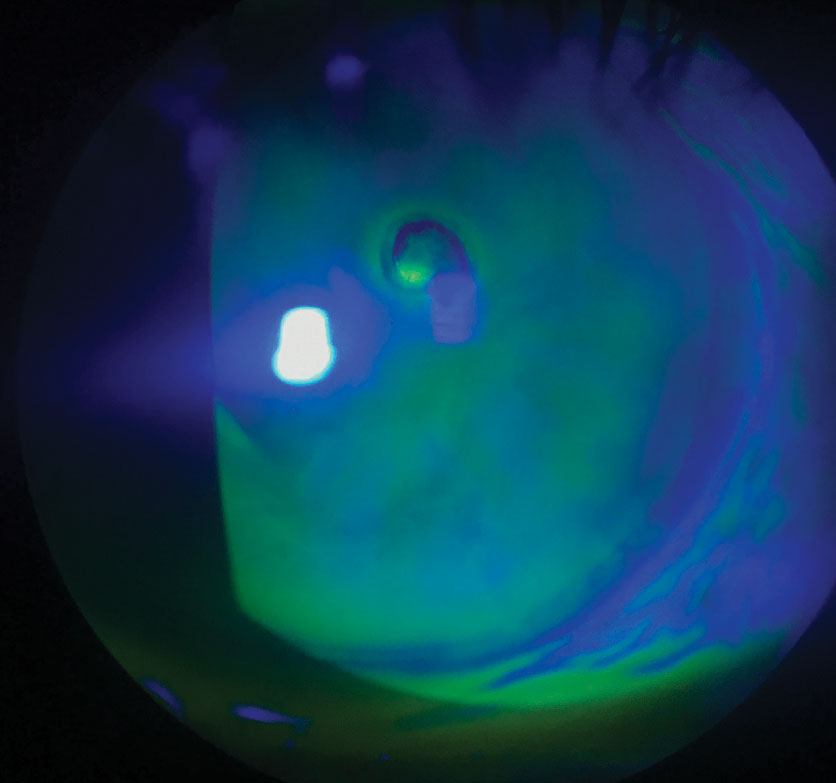 |
| This positive fluorescein staining shows a primal epithelial defect with healing margins and inferior pooling from RCE at the patient's second visit. |
Day One Do's and Don'ts
The epithelial cells must heal before you tin add together a steroid to control the inflammation. Almost often, once the defect is healed, the stromal edema volition resolve as well. At the patient's initial visit, place a bandage contact lens (BCL) for condolement. If chemosis is present, a lens with a base of operations curve of 8.6mm is usually necessary.
To prevent infection, apply a broad-spectrum antibiotic drop, such as a fluoroquinolone, until the next visit; however, it is inadvisable to utilise Besivance (besifloxacin 0.vi%, Bausch + Lomb) in the case of an epithelial defect due to the formulation of the pause. Besifloxacin 0.6% is formulated with DuraSite (InSite Vision), a polycarbophil, edetate disodium dihydrate and sodium chloride vehicle.i Be mindful of reported agin furnishings including corneal edema and glaucomatous damage.1,2 DuraSite blocks the trabecular meshwork and can be toxic to the ocular surface when used in medications prescribed at a big and intensive dose.2 Prescribed at low doses, drugs that incorporate DuraSite may cause corneal edema, inflammation and adverse effects fifty-fifty after only a single dose.3 The intermission has a bioadhesive delivery system, which allows for longer drug release time; therefore, it should be avoided in RCE patients.four
Starting treatment with i drop of a topical fluoroquinolone every two hours may be necessary if the chance of infection is higher. Reduce it to ane drop 4 times a solar day once the erosion begins to heal and until the BCL is removed.
Prescribing an oral antibiotic such as doxycycline 50mg (one tablet taken twice daily), aids the healing process and prevents the risk of perforation. Normally, you'd be concerned nearly perforation if an ulcer is present; however, even with RCEs, doxycycline can be an effective treatment aid.five By chelating metal ions that are structurally essential for the corneal epithelium, doxycycline irreversibly inhibits corneal matrix metalloproteinases (MMPs), such as MMP-ii activity since information technology is Ca2+ dependent, as the antibody partially extracts the tightly leap ion from the agile hemidesmosome site of the protein.6 In addition to inhibiting MMP activity, information technology likewise inhibits the synthesis of MMPs and proinflammatory cytokines, such as IL-1.6
The broad-spectrum antibody also kills migratory keratocytes responsible for the formation of scar tissue, which in plow allows full coverage of epithelial basal cells to form and the development of stratified epithelium. Researchers observed this at a minimum concentration of 100µm, which is like to that required in other tissues.6 In addition, past using doxycycline at a low dose of 50mg BID, the benefit is all the same seen without the negative side effects of gastritis and phototoxicity.
Be certain to ask the patient almost their job and daily activities. If they report that they're often in a dusty or dingy surroundings or engage in heavy lifting, it may exist necessary for them to await to return to work until the epithelium heals to lower the take a chance of infection. Once the epithelium is healed, the doxycycline tin can be discontinued; however, information technology is safe to go along the patient on the antibiotic for a full month or more at this low dose until the take a chance is minimized. Recommending over-the-counter pain relievers, prescribing a topical cycloplegic or suggesting a cold gel pack will also proceed the patient more than comfy.
Two-day Follow-Up
These patients need close monitoring and should render for a follow-up visit within two days. Be sure the patient knows to call if they experience any reduction in vision, every bit yous may want to see them sooner than scheduled. Removal of the BCL may exist necessary to fully assess the healing defect with subsequent staining of fluorescein. If the cells are nowadays but irregular, it may exist safe to just apply artificial tear lubrication, over-the-counter ointment QHS and continue the doxycycline for the full grade of handling. If the defect is still present, a replacement BCL should be placed on the centre; still, if the defect is larger or is not healing well, other treatment courses may be necessary.
Dealing with Complications
If the defect is boring to heal, or does heal simply the epithelium breaks downwards again, it's fourth dimension to plough to a complication protocol. Ordinarily, if the epithelium regresses, it does so following the removal of the BCL where the cells are not fully adherent all the same. In one study of thirteen clinically successful cases where an viii.6mm BCL was used for an chafe for an average of 24.9 hours, 5 cases had persistent corneal epithelial defects, despite clinical improvement or reported resolution of symptoms.7 Another showed that treatment with only a bandage contact lens had a 25% recurrence rate.8 If this occurs, consider using an amniotic membrane. This is used often in our practise to assistance the restoration of the epithelium faster while reducing the take a chance of haze.
Using Amniotic Membranes
Studies bear witness that amniotic membranes are helpful in the healing process through anti-inflammatory cytokines and peptides that promote tissue repair.8,9 They acheive this by reducing both inflammation and scarring as well as angiogenic actions (by inhibiting MMPs).8,9 Still, they are not considered a curative treatment.viii,ix
Currently, three manufacturers offering these products, which come in both dehydrated and cryopreserved forms, each with their own benefits and drawbacks. All the same, for a diagnosis of RCE, either membrane would support the epithelial healing process.10
The Prokera (Bio-tissue) is a cryopreserved amniotic membrane recognized for wound healing, inhibiting angiogenesis, reducing inflammation and minimizing corneal scarring and pain.11 Information technology has anti-inflammatory effects and contains neurotrophic factors that may promote corneal nervus regeneration.xi Due to its considerable diameter, it covers big areas of epithelial defects too every bit the limbus.11 Some patients may tolerate the large ring better with taping of the upper eyelid closed or partially closed. The product comes in Slim or Plus options. The Slim is slightly more than comfy for the patient and is therefore typically used initially. If the Slim dissolves in less than a week and the defect is nonetheless present, a Plus can exist used.
Follow-up should exist within four to seven days, giving the epithelial defect time to restore. If the defect is smaller or the patient cannot tolerate the band, a dehydrated membrane is a expert option.
The BioDOptix (Integra) is a dehydrated amniotic membrane that retains devitalized cellular components and has growth factors, such as vascular endothelial growth cistron (VEGF), platelet-derived growth factor and insulin-like growth cistron, as well as interleukins and tissue inhibitors of metalloproteases shown to attune inflammation.12,thirteen It comes in 2cm x 3cm or 1.5cm ten 2cm sizes.
To use this membrane, beginning lubricate the cornea with an artificial tear. Carefully catch the border of the membrane disc with a pair of jewelers forceps and place the stromal (dull) side of the disc down on the lubricated cornea over the epithelial defect. A pair of paddle forceps works best for this since the tips are flat, thus reducing the risk of tearing the membrane. If the cornea is lubricated well enough, the disc should immediately adhere to the surface and rehydrate on contact. Practice non try to shine wrinkles or bubbling if any are present. A BCL can and so be placed directly over the membrane for added protection and comfort.
The AmbioDisk (Katena) is as well a dehydrated amniotic membrane. The product comes in 9mm, 12mm and 15mm sizes. The membrane is preserved in a process known equally purion, in which key restorative elements such as epidermal growth factor, interleukin-10, VEGF and many others are preserved from their original state.xiv The allograft is placed with the basement membrane side downwards, next to a dry corneal surface, which can so be smoothed out with non-toothed forceps. A bandage contact lens or suture cloth tin can be used to allow the membrane to retain adherence to the cornea.
With any of these procedures, information technology is imperative that the patient keep the eye lubricated with preservative-free artificial tears, not only for comfort, merely for healing purposes. The patient's electric current antibiotic and steroid drop regimen is fine to proceed later on placing the membrane on the eye.
Research shows that using an amniotic membrane rather than a BCL allows the patient to potentially get longer before recurrence of the erosion. 1 study resulted in a 25% recurrence rate within i twelvemonth after a three-calendar month handling flow with a cast contact lens, while in a like written report, after treatment with an amniotic membrane, but a 10% recurrence charge per unit was seen within i year.viii,xv
If an amniotic graft is used, be certain to follow up within five to vii days, giving the membrane time to promote surface healing.
Near this Series
To aid optometrists strengthen their protocols for managing weather that require ongoing—perhaps life-long—care, this serial explains the steps to have after confirming a diagnosis, from day i through long-term management. Each installment in the five-part "Now What?" series will cover a unlike chronic status:
March—My Patient Has Glaucoma...Now What?
April—RCE
May—diabetic retinopathy
June—scleritis
July—AMD
Be certain to check www.reviewofoptometry.com for any articles y'all may have missed.
Fourth Follow-upward
At the five-to-seven day follow-up, if the epithelial defect is still present, identify another amniotic membrane; however, if the epithelium is healed just the cells are irregular, a bandage contact lens can give enough coverage for the epithelium to polish over until it is completely adherent. Throughout the procedure, lubrication is key, which should be stressed to the patient. In addition to the oral antibiotic and broad-spectrum antibiotic drop, using preservative-gratuitous bogus tears will support a healthy surroundings for the cornea to heal. Once the membrane or BCL is permanently removed, the patient should add an over-the-counter ointment at bedtime, such equally Muro 128 sodium chloride (Bausch + Lomb) ointment to preclude a breakdown of the epithelium overnight. Since Muro 128 ointment is a hypertonic agent, it provides better coverage and relief from any corneal edema present, while likewise being preservative-free, different other over-the-counter gels and ointments.
If inflammation is still nowadays or anterior stromal haze has adult, add a steroid such as loteprednol, fluorometholone or prednisolone acetate twice daily, until the inflammation has resolved and the brume is reduced. Even if a little inflammation and haze presists, one time the epithelium is nowadays, calculation a low-dose steroid has its benefits.16 Inquiry shows MMPs accumulate in tears of patients with any ocular surface illness and are mainly made from granulocytes.sixteen MMPs are especially abundant when accompanied past a coinciding systemic or autoimmune disease that involves ocular tissue and exacerbates an inflammatory response.16 At that place is a greater upregulation of MMPs in corneal disorders where collagen is destroyed and MMP-ii and MMP-9 are widely present in patients who have corneal melts and recurrent corneal erosions. Signaling of IL-6 is then activated which induces the inflammatory response of the corneal stroma.17
Steroid drops can exist used to command this cascade reaction by reducing inflammation, thus decreasing the amount of MMPs nowadays in the tear movie which then diminishes the trans-signaling of IL-6. Overall, when the tear picture has a minimal corporeality of MMPs present, epithelial adherence to the basement membrane is greatly increased.
A Recurring Diagnosis
The initial evaluation is key, as is gaining the patient'southward history of both the current episode and all prior ones. Since the erosions are a known diagnosis and are recurrent, it is important to re-examine the patient with a new perspective and capture any underlying atmospheric condition.
Instilling a Fluress or proparacaine drib will aid with the patient'southward comfort while you examine them. The story of an RCE is usually easily predicted: frequent eye pain upon awakening, with accompanying photophobia and epiphora. The patient may besides mutter of conjunctival injection, blurred vision and difficulty keeping their centre open. If there is accompanying EBMD or DED, the complaints may as well consist of asthenopia, fluctuating vision and burning, which more oftentimes occurs at the twenty-four hours's end.
Upon initial examination, staining with fluorescein may show a loss of epithelium, thus a positive epithelial defect, if the RCE is active. If the epithelial cells are healing past the time the patient appears for a visit, you may but see irregular epithelial cells in the place of the RCE, which can yet cause irritation and discomfort. If in that location is a defect, information technology should be measured, as this is how the healing process is quantitatively assessed and tracked. Annotation whether information technology is a true defect with positive staining of fluorescein or rather, pooling of fluorescein. If it is pooling, the epithelial cells are intact; even so, at that place may be stromal loss or a depression nowadays, which causes the pooling. If unsure, utilise a dry cotton fiber tip applicant to soak upwards the fluorescein; if no staining is seen, the epithelial cells are fully intact; still, if the expanse re-stains, an epithelial defect is nowadays. Exist sure to besides note the amount of inflammation present: is in that location conjunctival injection only or are their stromal folds and inflammation underlying the epithelial defect as well? Are fine keratic precipitates visible with an anterior chamber reaction and is the upper lid showing erythema and edema as a protective reaction to the erosion?
Pay attention to the size, shape and design of the eroded epithelium. Stained tracks among the corneal epithelium are an indication to evert the upper eyelid to bank check if a foreign body is present, which would change the diagnosis from a truthful RCE. If the patient has tried to suffer the erosion without handling for several days, more of an inflammatory response is expected. This also puts the patient at a college risk for infection. Do not allow an overabundance of inflammation steer you away from the proper initial form of action, and exist certain to notation whatever signs of infection, such every bit infiltrates or an ulcer, before proceeding with treatment, as this would drastically alter your course of treatment and direction.
Getting to the Root
ODs must accost the underlying condition of the recurrent erosion, whether information technology's previous trauma, EBMD or a grade of chronic OSD (due east.g., ocular rosacea, blepharitis, meibomian gland dystrophy, exposure keratitis).
Practise not forget to examine the fellow eye closely, every bit some erosions tin exist thought to take only occurred from previous trauma when the patient really has EBMD. This is an autosomal dominant condition where signal mutations in the TGFBI gene on chromosome-5 are considered responsible for some erosions. EBMD can also be known equally map-dot-fingerprint dystrophy, Cogan's microcystic dystrophy or anterior basement membrane dystrophy. In this dystrophy, extra sheets of basement membrane extend abnormally into the epithelium. In plow, the epithelium growing anteriorly becomes entrapped in the extra sheets causing clumping and poor adherence.18 This can cause poor vision, constant discomfort and foreign body awareness, glare and halos, and of class recurrent corneal erosions. If there is previous anterior stromal haze or scarring from trauma or numerous erosions, the prognosis for a proficient effect may decline. Often, if there is already corneal haze and scarring, the epithelium may not heal well. Likewise, if DED is a gene, the epithelial cells may regenerate at a slower rate, which increases the run a risk for the epithelium to break downward and heal with rest anterior stromal brume or scarring.
In nearly cases, the RCE will go on to occur unless the underlying status is managed and addressed. Moreover, in that location tin can be more than i etiology, as many times EBMD and DED are both collaborating factors in the recurrent erosions. Prescribing a dry heart drib such every bit Xiidra (lifitegrast, Shire) or Restasis (cyclosporine, Allergan), along with 2,000mg daily dose of omega-3 fatty acids will help reduce whatsoever unwarranted inflammation of the lid margin. Therapy tin can too include warm compresses with chapeau massage, artificial tears four to six times daily, and Muro 128 ointment at bedtime. If inductive blepharitis is diagnosed, lid hygiene will need to be discussed as well.
Avenova spray is a smashing tool for the lid margin, forth with tea tree oil shampoo (for Demodex) or over-the-counter lid scrubs. For more than severe cases, autologous serum can be prescribed, which is compounded from the patient's own blood. The serum contains a mixture of growth factors and cytokines, similar to the human amniotic membranes, and should be kept cold at all times while being dosed every two hours while awake.19 Inquiry shows that by addressing the DED, the incidence for recurrent erosions are significantly reduced.19
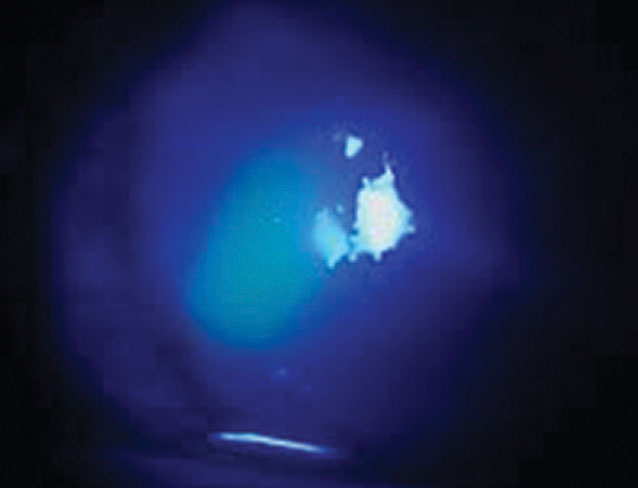 |
| This active RCE, seen with positive fluorescein staining, shows an epithelial defect nasally, measuring 1.5mm x 2.4mm. |
Lifestyle Changes
Patient teaching plays a large role in non only the healing of an RCE but too the prevention of one. The patient needs to understand that corneal erosions tin can be an ongoing effect and may not ever have the best outcome if severe enough. Employ the explanation that the surface peel cells of the cornea have sloughed off because they are loose and non-adherent; this creates a visual for the patient to better understand.
Once healed, it is important to prevent further episodes from occurring, which is why clinicians prescribe dry out eye therapy, especially the ointment at bedtime. After the patient understands the importance of the prophylactic handling, they are much more willing to be compliant.
The difficulty comes, however, when the patient does not heal well and has balance anterior stromal haze affecting the quality of the vision. Sometimes all that is needed is an updated spectacle or contact lens prescription or the use of a low-dose steroid for several weeks to minimize the haze. During the management of an RCE, if the patient is non healing well, starting the chat early on is beneficial, every bit their expectations volition be realistic for the final visual outcome. Reassure them that you are applying every measure for a good issue and stress the magnitude of the rigorous drop schedule. If the haze is severe, at times, a specialty contact lens such every bit a scleral or hybrid lens tin can help the patient gain better best-corrected vision. The quality of the tear film should never exist taken for granted, as it can greatly enhance the vision, especially if there is residual haze; therefore, handling for dry center disease should exist initiated.
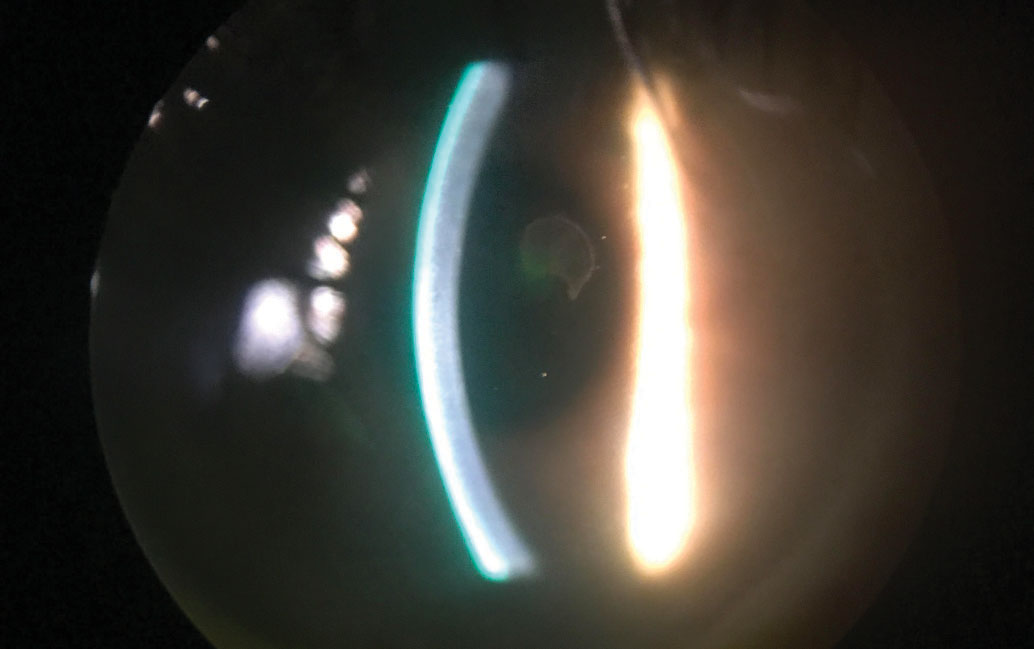 |
| This patient has a central epithelial defect with healing margins. It'southward slightly difficult to discern whether it is a truthful defect without fluorescein staining. Click image to enlarge. |
Surgical Intervention
If the erosions continue and medical treatment fails, a surgical procedure may be necessary. Clinicians may need to coordinate with local corneal specialist; however, depending upon the process, some tin be completed in-office.
Anterior stromal puncture (ASP) is a handling that is useful for RCEs that occur in the peripheral cornea and can be done in the examination lane. Due to the run a risk of corneal scarring, it is not recommended when the erosion is central or mid-peripheral. Superficial punctures are made with a 25- or 27-approximate aptitude needle, piercing the epithelium to Bowman's layer in 0.5mm spot treatments. This can also be done using a Nd: YAG laser, giving short bursts of energy to the cornea, which are more than repeatable and shallower, thus diminishing the amount of scarring created than if by hand.19 In one review, ASP did have a recurrence charge per unit of 40% and needed boosted treatment.20
Epithelial debridement is also an in-office process that is commonly done, in which a Merocel spear and blunt spatula are used to remove the central 7mm to 10mm of loose, central epithelium.xix A bandage contact lens or an amniotic membrane can then be placed on the middle, forth with the appropriate drop regimen; however, due to the loftier recurrence rate, this procedure is usually combined with extra steps.
Superficial keratectomy (SK) is an out-patient process, usually done in the operating room, in which the loose epithelial cells are removed with a Merocel spear, ensuring that the eye is not undertreated. This is then followed by treatment of the underlying basement membrane with a diamond burr which rejuvenates the membrane to allow potent, anchoring adhesions to the new epithelial cells when healing.21 Afterward the SK, the postoperative care direction in regards to lubrication and the BCL or amniotic membrane will exist similar to the treatment and management for an RCE. The patient volition also exist on a soft steroid, antibody and NSAID taper schedule over several weeks.
Phototherapeutic keratectomy (PTK) is another common surgical option in which the epithelium is removed either by hand or an argon fluoride excimer laser. The laser is so used to emit ultrashort pulses of 193nm to ablate the irregular areas and opacities on a submicron level of Bowman'southward layer and the outer 5µm to 7µm of the stroma, without damaging the middle stroma.22 This allows for the epithelium to regrow and form stiff adhesions to the anterior stroma.19
PTK is widely used for corneal opacities, such every bit corneal scars, Salzmann's nodular degeneration, recurrent erosions and EBMD. This procedure with the excimer laser removes enough of the superficial Bowman's layer to permit formation of a new basement membrane with stronger adhesion structures.22 The postoperative treat PTK is the same as with SK.
It is important to continue all physicians caring for the patient (due east.g., referring doctor, primary care doctor, rheumatologist) informed of the diagnosis and treatment. Many underlying conditions can bear on the wellness of the ocular surface, especially autoimmune diseases, such as rheumatoid arthritis, systemic lupus erythematosus, or diabetes mellitus. If the patient has one of these medical conditions, they can be expected to heal slower and may need to be monitored more than closely every bit it is not uncommon to hitting a roadblock during the treatment process.
When writing a letter, be sure it is informative merely succinct. It should include the diagnoses, treatment and direction, every bit well as your concern for healing in relation to the patient's systemic weather. Information technology is always beneficial to stand for with other physicians as this opens the path of friendly communication between colleagues, assuasive them to know yous tin can be a reliable referral source and have the patient's all-time involvement in heed.
Other considerations to go on in listen are whatever systemic medications that the patient may already be taking that could inhibit the healing process of the erosion. Medications such as antihistamines, anticholinergics or anxiolytics and antidepressants are commonly prescribed and cause extra overall dryness, as well as ocular surface dryness and irritation. Be sure to view the entire picture and recognize what handling is best suited for that particular patient.
Recurrent corneal erosions are common and are something that we, every bit clinicians, tin can care for and manage. At that place are many handling options from over-the-counter ointments to prescription drops and oral medication, from bandage contact lenses to human amniotic membranes, as well every bit many environmental additions that can all help in the healing of RCEs.
Dr. Finch Crouch is an optometrist at Eye Centers in Louisville, Kentucky.
acostagailintence.blogspot.com
Source: https://www.reviewofoptometry.com/article/my-patient-has-recurrent-corneal-erosionnow-what
0 Response to "Can Night and Day Contact Lens Heal Erosion"
Post a Comment